Attention Deficit Hyperactivity Disorder (ADHD) is conventionally conceptualised as a neurodevelopmental disorder of attention and executive control. However, in adult clinical populations — ADHD does not travel alone. Instead, it is repeatedly embedded within a broader pattern that includes sensory overload, autonomic lability, hormonal sensitivity (women), connective-tissue-leaning features, immune and histamine reactivity, metabolic vulnerability, increased muscle tension, and difficulties with interoception and emotional labelling. These features recur with striking consistency, even in individuals who do not meet strict thresholds for hypermobility syndromes or overt dysautonomia on standard screening tools and is particularly noticeable among women presenting in midlife.
The High-Gain Regulatory Phenotype
This essay proposes that approximately 5% of humans occupy the high end of a conserved regulatory phenotype characterised by fast signalling, reduced biological damping, and heightened responsivity across neural, autonomic, endocrine, immune, and connective tissue systems.
ADHD represents the cognitive–behavioural expression of this architecture; associated somatic and affective features are downstream consequences of the same regulatory design rather than coincidental comorbidities. This phenotype appears optimised for early-life adaptability and situational responsiveness, but carries predictable costs in modern environments defined by longevity, sedentary work, chronic psychosocial stress, and prolonged hormonal cycling.
Rather than framing these presentations as collections of unrelated disorders, we should treat them as expressions of a single underlying physiological strategy — one that is adaptive under certain conditions, and destabilising under others.
ADHD as a Disorder of Translation Rather Than Attention
In clinical practice, the core impairment in ADHD is often not sustained attention per se, but translation: the effortful conversion of signal into meaning, intention into sequence, and internal state into language. Many individuals with ADHD can attend intensely under conditions of novelty or urgency, yet struggle to process verbal or auditory information, initiate or organise action in low-pressure contexts. This pattern reflects difficulty with semantic sequencing and prioritisation rather than inattentiveness.
Language processing difficulties are common and often well masked, particularly in verbally fluent adults. Listening fatigue, difficulty processing spoken information in groups, and reliance on visual or kinaesthetic cues are frequent and hidden, with significant shame attached.
These same individuals often struggle to identify or label internal emotional and physiological states in real time, despite high cognitive insight. Alexithymia-adjacent profiles and reduced interoceptive access are therefore common, not as primary deficits but as secondary consequences of a system biased toward external scanning and rapid response rather than inward monitoring.
This translation bottleneck provides a conceptual bridge between ADHD, sensory overload, emotional dysregulation, and delayed recognition of exhaustion or overwhelm.
A High-Gain, Low-Damping Regulatory Architecture
Across multiple physiological systems, individuals at the high end of this phenotype exhibit a pattern of fast responsivity with limited buffering. Neural signalling is rapid and flexible but prone to noise; autonomic responses mobilise quickly but settle slowly; immune and mast-cell activity is vigilant but easily triggered; connective tissues show compliance rather than rigidity; hormonal fluctuations exert outsized effects on cognition and affect.
This can be described as a high-gain, low-damping regulatory architecture. Inputs are amplified efficiently, but the system struggles to stabilise once activated. Such an architecture favours speed, sensitivity, and adaptability, but trades away endurance and long-term equilibrium.
Crucially, this model does not require a single gene or syndrome. Polygenic traits affecting neurotransmission, extracellular matrix properties, immune signalling, and endocrine sensitivity naturally co-aggregate because they are expressions of the same regulatory strategy at different biological scales.
Why Only 5% of Humans?
Traits that are both costly and situationally advantageous tend to stabilise at low but persistent frequencies. Evolution does not optimise individuals for comfort or longevity; it optimises populations for survival under variable conditions. A phenotype that confers advantages in uncertain or dangerous environments — but incurs energetic, metabolic, or injury costs — will not spread universally, nor will it be eliminated.
Approximately 4–6% represents a plausible equilibrium for such a specialist phenotype. Below this, its group-level benefits (early threat detection, rapid mobilisation, innovation under pressure) would be lost; above it, group cohesion and efficiency would suffer due to excessive volatility. Importantly, this estimate does not rely on historical prevalence measurement — which is impossible — but on well-established principles of evolutionary trade-offs in polygenic traits.
Sex Differences and Hormonal Stress-Testing
Men and women share this underlying regulatory architecture, but its expression diverges due to hormonal modulation. Oestrogen amplifies dopaminergic, glutamatergic, immune, and histamine signalling, while progesterone provides a key GABAergic brake. In women, cyclical hormone fluctuations therefore act as repeated stress tests of system stability.
Historically, frequent pregnancy and prolonged lactation would have reduced lifetime exposure to hormonal cycling, and most women would not have lived into perimenopause. In modern contexts — characterised by low parity, decades of menstruation, and extended lifespan — the stabilising buffers are removed. As a result, latent vulnerabilities are exposed, often dramatically, in the late 30s and 40s. Premenstrual dysphoria, perimenopausal cognitive collapse, and heightened sensory and autonomic symptoms should therefore be understood as revelatory, not causative.
Men express the same phenotype through different downstream risks: addiction vulnerability, burnout, cardiovascular and metabolic disease, and autonomic instability without the hormonal amplification seen in women.
Life-History Optimisation and the Cost of Longevity
This phenotype appears optimised for early-life performance rather than long-term durability. Connective tissue compliance may reduce obstetric risk by facilitating pelvic flexibility, but at the cost of postpartum recovery and later musculoskeletal stability.
Autonomic vigilance enhances survival in dangerous environments but becomes maladaptive when threats are chronic, symbolic, and non-actionable. Metabolic flexibility supports rapid energy mobilisation but predisposes to insulin resistance in conditions of abundance.
Evolutionary selection pressure drops sharply after reproduction. There is little evolutionary penalty for pelvic floor dysfunction, chronic pain, or metabolic disease emerging decades later. Modern medicine, by contrast, implicitly assumes bodies are designed for prolonged healthspan, and therefore misclassifies predictable trade-offs as pathology.
Interoception, Alexithymia, and Symptom Under-Reporting
Reduced interoceptive access may be an adaptive corollary of this phenotype. In environments requiring rapid external response, excessive inward attention would be costly. Delayed or muted perception of internal states allows action to take precedence over reflection. In modern clinical contexts, this shows as difficulty describing symptoms or calibrating symptom severity, under-reporting on questionnaires, and late presentation when physiological load finally exceeds coping capacity.
This explains the frequent mismatch between low self-reported autonomic or sensory scores and significant clinical impairment. Standard tools measure conscious symptom perception, not physiological burden.
Implications for Treatment Response and Clinical Practice
Understanding ADHD as part of a broader regulatory phenotype reframes midlife deterioration not as psychological failure (what we ADHD-ers tend to think), but as the predictable consequence of prolonged mismatch between ancient physiology and modern demands.
It also has practical consequences. Reframing ADHD as the cognitive expression of a broader high-gain regulatory phenotype has had marked implications for treatment response in my clinical practice. When ADHD is treated in isolation, stimulant response rates are often reported at around 50–60%, with discontinuation commonly attributed to “side effects” such as anxiety, insomnia, headache, emotional flattening, gastrointestinal disturbance, or a sense of being overstimulated.
Maybe it’s not them, it’s us?
As an ADHD doctor, with ADHD, on treatment, I am both them and us of course, but what is important here is that within the framework proposed here, many of these “side effects” are better understood as predictable consequences of introducing dopaminergic agents into an already dysregulated physiological system.
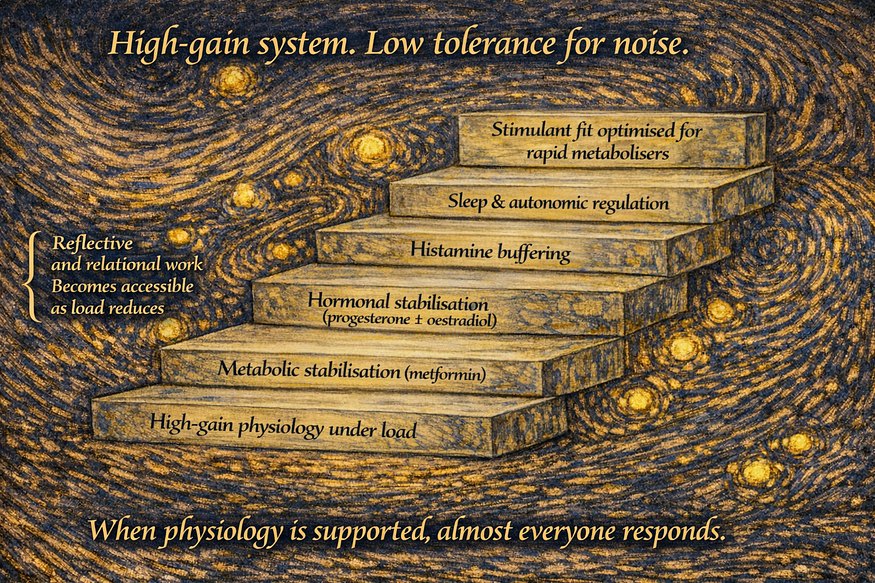
In this phenotype, apparent stimulant “side effects” frequently reflect unrecognised hormonal volatility, metabolic instability, autonomic sympathetic overdrive, histamine reactivity, or high sensory gain combined with reduced interoceptive access. When these factors are left unaddressed, stimulant initiation can amplify discomfort rather than reduce cognitive load. By contrast, when treatment is embedded within a broader physiological scaffolding approach — attending to sleep anchoring, autonomic tone, hormonal stability, hydration and metabolic rhythm — tolerability and effectiveness improve substantially.
Towards 100% treatability?
In my ADHD clinic, adopting this integrated approach has shifted meaningful treatment response from approximately half of patients to the vast majority. This does not imply that every individual tolerates every medication, but rather that nearly all patients derive clinically useful benefit once treatment is paced, contextualised, and titrated with attention to physiological stabilisation and regulatory load.
Key principles include starting at very low doses, increasing slowly, introducing one intervention at a time, and prioritising subjective calm and reduction in internal noise before expecting gains in executive function or productivity. In this population, calm is often the earliest and most reliable marker of appropriate dosing; function follows once physiological threat is reduced.
This approach also requires recognising that individuals with reduced interoceptive precision may struggle to articulate early signs of overload. Treatment decisions therefore benefit from careful observation of sleep quality, muscle tension, sensory tolerance, and end-of-day fatigue, rather than relying solely on self-reported symptom scales. When dosing is guided by these signals, stimulants frequently improve language processing, cognitive translation, and emotional steadiness without provoking the adverse effects that previously led to discontinuation.
Taken together, these observations suggest that variability in ADHD treatment response is not solely a property of the medication or the diagnosis, but of the physiological context into which treatment is introduced. Addressing the broader regulatory phenotype transforms both tolerability and outcome.
Just my clinic folks..…
This model does not claim genetic determinism, uniform expression, or universal applicability to all ADHD presentations, but I am talking about everyone in my ADHD clinic. It does not provide historical prevalence estimates or identify a single causal pathway. Rather, it offers a unifying framework that accounts for repeated clinical clustering across systems, plausibly explains why these features co-travel so reliably in a subset of individuals and gives important suggestions to optimise treatment.
TLDR summary
So approximately 5% of humans appear to occupy the high end of a conserved regulatory spectrum optimised for speed, sensitivity, and adaptability rather than stability or longevity. ADHD represents the cognitive expression of this architecture; associated somatic, hormonal, autonomic, and metabolic features are downstream consequences rather than independent disorders. In modern environments, this phenotype is increasingly exposed, misunderstood, and medicalised. A regulatory, life-history-informed framework offers a more coherent and humane understanding — and points toward more effective clinical support.